

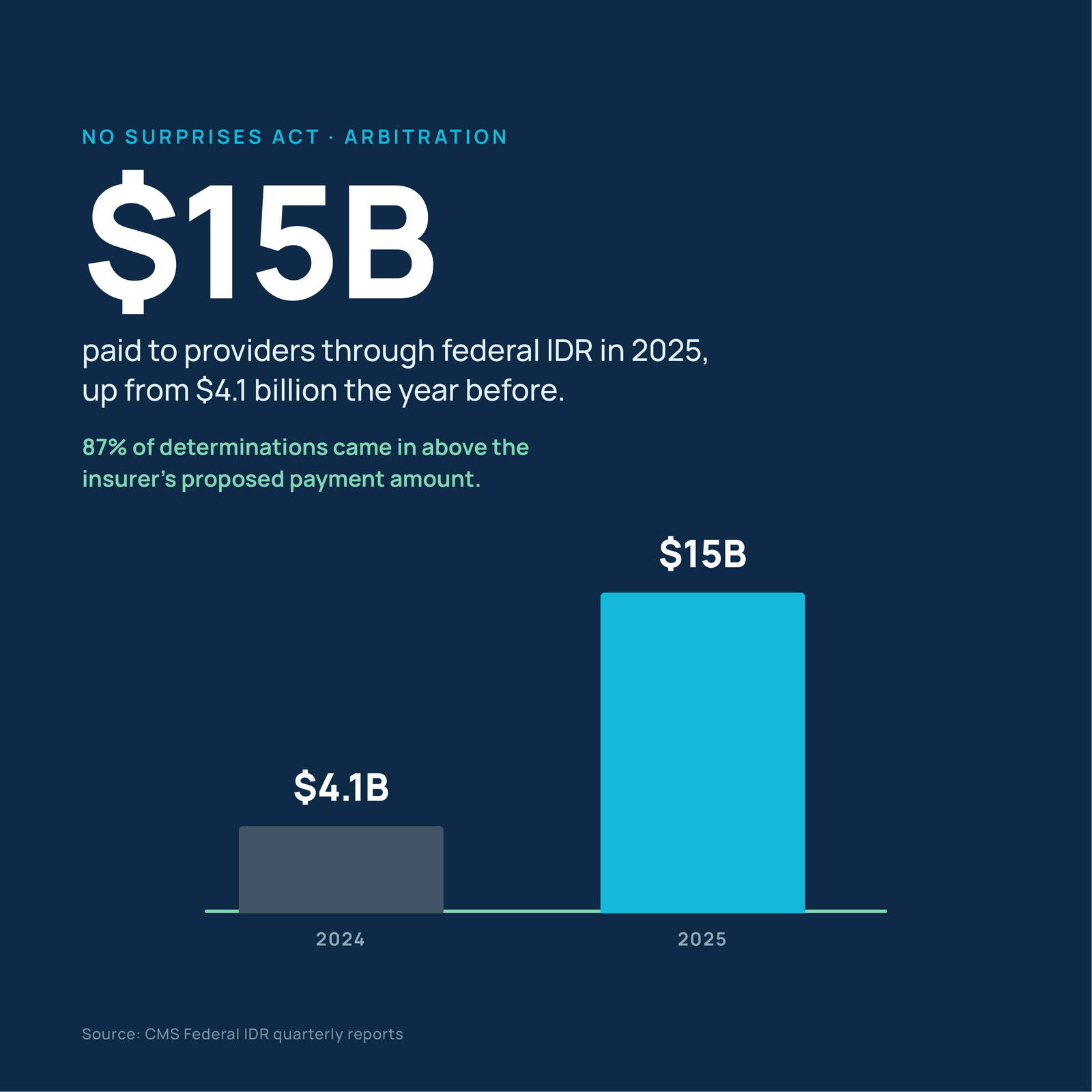
No Surprises Act Arbitration Paid Providers $15 Billion Last Year. I Wouldn't Build a Budget on It.
Providers pulled roughly $15 billion out of No Surprises Act arbitration last year, up from $4.1 billion the year before, and they're winning 87 percent of determinations. I've been chewing on that win rate all week, because a number that high in an adversarial process isn't a competitive advantage. It's a signal the process is mispriced, and mispricings in healthcare payment don't last.
Medicare Just Asked Whether AI Should Change What a Doctor's Visit Is Worth
Most of the coverage of the 2027 Medicare rule stopped at the rate cut. Further in, past the tables, Medicare stops proposing things and starts asking questions. One of them: if technology does part of the work of a primary care visit, how much should the visit be worth? Nobody has asked that in a payment rule before, and it will matter more to your revenue cycle than the rate cut will.
Follow the Money: The Smart Capital Already Voted on What 2030 Looks Like
While hospital strategic plans debate AI pilots, private equity signed a $12 billion revenue cycle deal, Ascension bought 300 surgery centers, and investors stopped counting AI as a differentiator. The capital already voted on what 2030 looks like.

602 Hospitals Are Already Underwater. Here's What CFOs Need to Do Before the Next Wave Hits.
Six hundred and two hospitals are already running a combined $10 billion deficit, and that's before a single federal cut has landed. I read the full report, the appendices too, so you don't have to. Here's what's advocacy framing versus hard CMS data, and the three things your board needs to hear before this shows up as next quarter's bad news.

Every State Is Writing Its Own AI Rulebook. Washington Hasn't Started.
34 AI healthcare laws passed in 21 states in 2025 alone. Here's what CFOs and RCM leaders actually need to do about the patchwork, before Washington ever weighs in.

I Forecast the Future of Revenue Cycle Management From a Travel Company. Here's Why That Makes Me Better At It.
I forecast the future of the revenue cycle from a travel company — no hospital in sight. That's not as strange as it sounds. The reason I can see where RCM is headed has little to do with being in healthcare and everything to do with no longer being buried alive in it. A piece about altitude, thinking time, and the industry that quietly steals both from the leaders who need them most.

Why Revenue Cycle Efficiency Won't Save Hospitals From Structural Revenue Loss
Every hospital is fighting the same fire right now: denials, rework, coding, labor cost. Good. But there's a second fire in the building, and almost nobody is pointing a hose at it. Operational efficiency and structural revenue loss are two different problems, and you can't automate your way out of the second one.
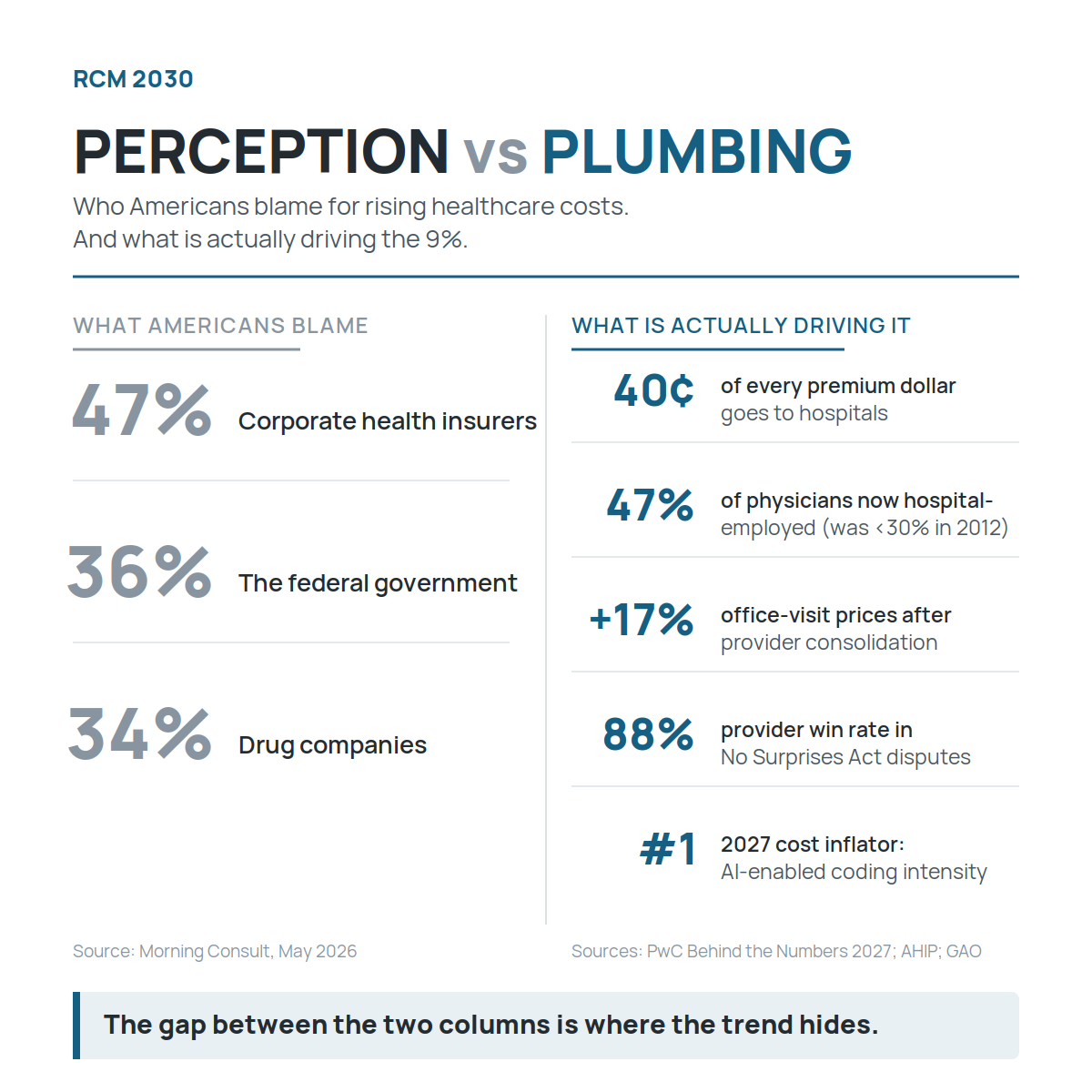
The Enemy Is Us. And AI Won't Be the Hero.
We keep looking for someone to blame for rising healthcare costs, and we keep hoping AI will rescue us. After most of a career in the revenue cycle, I think both instincts are getting in the way of the work that actually moves the number. Here is why.

AI and the Revenue Cycle Workforce: What This Week's Healthcare News Means for Staffing in 2030
Will AI replace revenue cycle jobs; AI revenue cycle staffing 2030; RCM workforce modernization; healthcare AI layoffs revenue cycle; deskilling revenue cycle; new RCM roles AI

Why Does AI Keep Creating More Work for My Revenue Cycle Team?
Automation doesn't shrink your revenue cycle team; it changes what they have to be good at. Here is why AI is creating more work, not less, and what hospital CFOs should do about it before 2030.
The Problem Isn't That Hospitals Are Moving Too Slow. It's That They Think Slow Is Fine.
Three flavors of AI laziness are quietly stalling hospital revenue cycles right now: the pilot that never ends, the checkbox deployment, and the assumption that your vendor handles it. This week proved the runway is shorter than most leaders think. Here is the honest 2030 forecast and the one thing worth doing before your next leadership meeting.
The AI Lawsuits Are Here. What Should RCM Leaders Do Before the Next One Names Their Hospital?
Pennsylvania just sued an AI chatbot for impersonating a licensed physician. UnitedHealthcare faces a class action over an algorithm plaintiffs say has a 90% error rate and was used to override physician judgment without human review. Both cases are being treated as consumer tech and payer problems. They are not. Every legal theory being established in these lawsuits applies directly to how hospitals use AI in prior authorization, denial routing, and charity care screening right now. Here is what CFOs and RCM leaders need to do before the next lawsuit names a provider.
Will RCM Vendors Survive the AI Revolution? What Waystar's Big Quarter Actually Tells Us About the Future of the Vendor Landscape
Waystar posted 22% revenue growth in Q1 and said out loud what most vendors only say in board decks: they are building toward automating a meaningful portion of the $100 billion in annual RCM labor pool. That is excellent marketing. It is also a market thesis about your headcount, your vendor contracts, and what the revenue cycle looks like in 2028 — and most CFOs and PE firms are not asking the right questions about what it means yet.

When Your AI Agent Goes Slowly Crazy: What Revenue Cycle Leaders Need to Know Right Now
Rush University Medical Center is 18 months into its agentic AI journey. What they learned should be required reading for every CFO and revenue cycle director in the country. The problem with agentic AI isn't that it breaks. It's that it drifts, slowly, quietly, in directions nobody notices until the damage is already in your A/R. Here's what that means for your revenue cycle and what to do about it.

My Predictions Were Right. That's Not the Good News.
I stopped writing RCM 2030 for three weeks when the reconciliation bill passed. Not because I was stuck, but because I had to rethink what I'd written about 2027 and beyond. The Senate just passed a budget resolution with reconciliation instructions due May 15 and hundreds of billions in unspecified cuts to find. This week's news tells me the trajectory I described is exactly right. Here's what the book predicted and what's actually happening.

Healthcare Is Under Pressure. AI Won’t Save It by Itself.
Hospitals are facing pressure from multiple directions at once. Medicaid funding is tightening. Amazon continues expanding its healthcare footprint. And behind the scenes, many health systems are quietly abandoning AI pilots that never delivered real results.
These forces might look unrelated, but they all converge in one place: the revenue cycle. As margins tighten and expectations rise, finance leaders are being pushed to separate real operational transformation from technology hype. The next few years will determine which organizations turn AI and automation into real financial resilience and which ones get left managing the wreckage of failed experiments.
The RCM Workforce Trap: Why Cutting Jobs and Outsourcing Without Oversight Is a Slow-Moving Disaster
Three health systems cut RCM and IT jobs this week. Some of those decisions will age well. Others won't. April Wilson breaks down what organizations get wrong when they outsource without keeping internal oversight — and what the ones getting it right are doing differently.

AI Is Reshaping the Healthcare Workforce
Artificial intelligence is beginning to reshape the healthcare workforce itself. From AI scribes training new physicians to shifting workforce roles and the end of healthcare’s AI experimentation phase, revenue cycle leaders should start preparing their teams for a fundamentally different operational environment.
Payers Are Using AI Against You. Here's What It's Costing You Right Now.
UnitedHealth just deployed 22,000 engineers on AI. Payer recoupments are growing at twice the rate of claims. A new federal fraud enforcement division just launched. Here's what this week's news means for your revenue cycle.

AI Governance Is Coming to Healthcare
Artificial intelligence is moving quickly into healthcare operations. Ambient documentation tools are listening during visits, AI systems are influencing claim workflows, and predictive models are shaping payer decisions.
Now policymakers are starting to respond.
From state legislation targeting AI-driven claim denials to policy recommendations from major EHR vendors, a new phase of healthcare AI is emerging. Governance.
For revenue cycle leaders, this is more than a regulatory debate. AI is increasingly embedded in the workflows that determine how claims are documented, coded, and reimbursed. That means policy decisions about automation could directly affect hospital margins and operational strategy.